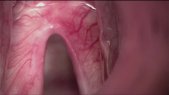
In this video we show a total laryngectomy. The most commonly followed incision for total laryngectomy is the U-shaped incision. If possible, the tracheostomy incision is made separately. The subplatysmal flap is raised superiorly above the level of hyoid bone and inferiorly up to the level of the sternum and clavicular heads. We liberate the specimen by sectioning the strap muscles and the omohyoid muscle inferiorly and dettaching the suprahyoid muscles from the hyoid bone superiorly. How the thyroid is dealt with depends on the extent of the tumor. Once the thyroid is out of the way, we continue to separate the tissues from the specimen laterally. We cut the constrictor muscles out of the thyroid cartilage. We then cut the mucosa over the epiglottis and once the epiglottis is identified we grasp it and retract it with the specimen. To avoid cutting through the tumor or its submucosal extension, the pharynx may be entered contralateral to the tumor. Once the extent of the tumor can be assessed through the opened pharynx, we continue to complete the upper limit of the dissection cutting the pharyngeal mucosa. On the lower end, we create the stoma cutting between two tracheal rings and we then separate the trachea and larynx from the esophagus. Once the specimen is out, we carry out the pharyngeal closure, which is a critical step. Finally we end up creating the stoma and closing the entire wound by layers.














0 Comments
There are no comments yet. Add a comment.